Though Gustav is presently Category 3 -- it is expected to strengthen overnight. The first 100-plus-mile-an-hour-winds will likely make landfall near New Orleans at dawn, tomorrow. It must seem almost too much to bear for all the Katrina survivors. . . .
Keep all in the path -- from the bottom of the Netherland Antilles, to Cuba, to the U.S. Gulf Coast -- in your meditations, overnight:
Latest available NOAA updates.
Sunday, August 31, 2008
Our Thoughts, Meditations and Prayers Turn to the Gulf Seaboard. . . .
Saturday, August 30, 2008
And, Speaking of Getting a Lil' [More] Help from Merck: What was VYCTOR?
UPDATED -- 09.04.08 @9 AM EDT
~~~~~~~~~~~~
And now, just to be complete -- I have put up a new post on this topic.
END UPDATED PORTION
~~~~~~~~~~~~
Perhaps Dick Clark and Co. would like to explain why this study, called VYCTOR, involving Vytorin -- was completed in December 2005 -- but was apparently only logged-in, and made public, at ClinicalTrials.gov (Identifier NCT00738296), two weeks ago -- on August 18, 2008.
A HUGE Hat Tip, to PM -- again! -- for a fabulous find!
Stay-tuned -- As I will likely have more on this, by Tuesday afternoon.
Friday, August 29, 2008
Vytorin Joint Venture Governance Agreements: To Be Kept "Secret" Until December 31, 2015?
I confess that I remain puzzled as to how, exactly, Schering's SEC lawyers believe their client is even remotely in compliance with the applicable portions of Item 601. The general rule is that each company must file (or incorporate) a complete set of exhibits for itself, for each filing it makes (and incorporation from other non-affiliated companies' filings is not permitted) -- particularly related to Exhibit 10 -- Material Contracts, under SEC Regulation S-K -- specifically Instruction 2, to Item 601 -- when it comes to disclosing what is perhaps the single most material of all the amendments to all of the contracts to which Schering-Plough is presently a party, viz.:
. . . .Material contracts.
Every contract not made in the ordinary course of business which is material to the registrant. . . .
. . . .Instruction 2. In any case where two or more indentures, contracts, franchises, or other documents required to be filed as exhibits are substantially identical in all material respects except as to the parties thereto, the dates of execution, or other details, the registrant need file a copy of only one of such documents, with a schedule identifying the other documents omitted and setting forth the material details in which such documents differ from the document a copy of which is filed. The Commission may at any time in its discretion require filing of copies of any documents so omitted. . . .
Instruction 2 to paragraph (b)(10): If a material contract is executed or becomes effective during the reporting period reflected by a Form 10-Q or Form 10-K, it shall be filed as an exhibit to the Form 10-Q or Form 10-K filed for the corresponding period. See paragraph (a)(4) of this Item. With respect to quarterly reports on Form 10-Q, only those contracts executed or becoming effective during the most recent period reflected in the report shall be filed. . . .
So -- why, again, aren't the Cholesterol Governance Agreements filed as exhibits, or at least summarized in a schedule attached to Schering's most recent Form 10-Q?
And now, add, on top of all of this, that I guess we'll all be in the dark for quite a while: we won't find out what those confidential portions -- as filed by Merck last month -- provide, until the beginning of 2016. Doubly odd:
. . . .Merck & Co., Inc. submitted an application under Rule 24b-2 requesting confidential treatment for information it excluded from the Exhibits to a Form 10-Q filed on July 31, 2008.
Based on representations by Merck & Co., Inc. that this information qualifies as confidential commercial or financial information under the Freedom of Information Act, 5 U.S.C. 552(b)(4), the Division of Corporation Finance has determined not to publicly disclose it. Accordingly, excluded information from the following exhibit(s) will not be released to the public for the time period(s) specified:Exhibit 10.1 through December 31, 2015
Exhibit 10.2 through December 31, 2015
Exhibit 10.3 through December 31, 2015
Exhibit 10.4 through December 31, 2015
For the Commission, by the Division of Corporation Finance, pursuant to delegated authority:
/s/ Patti J. Dennis
Chief, Office of Disclosure Support
Truly puzzling, that.
Again, Via a Tip From PM: DoD to Share Data with FDA -- Investigating Possible Vytorin-Cancer Links
PM (once again!) alerted us to a salient article -- more follow-up on the SEAS Vytorin-cancer data. While the full-version requires registration -- Therapeutics Daily offers a summary, for free, telling us all we really need to know:
The US FDA is aggressively tracking down all possible leads. Quoth the summary:
. . . .The Department of Defense is searching its medical database at FDA's request to investigate a potential link between cancer and the cholesterol-lowering drug Vytorin. The investigation is an example of FDA and DoD sharing more medical information and expertise in recent months, a DoD official says.
DoD is researching TRICARE for cancer diagnosis codes and the medications prescribed, says Rear Adm. Thomas McGinnis, a former FDA official who is responsible for TRICARE'S pharmacy operations. The investigation is intended to last nine months. . . .
[Emphasis supplied.]
This is the sort of diligence -- and active inter-agency cooperation -- our tax-dollars should garner, when public health and welfare might be at stake.
Thursday, August 28, 2008
Scheduling Updates -- in the Schering Clarinex® (Descloratadine) Patent Lawsuits
First, by agreed order, Schering's reply to the Sandoz motion to dismiss is now due on September 9, 2008 (it was to be due August 26, 2008). [You'll recall that this suit, In Re Descloratadine Patent Litigation (MDL No. 1851, Case No. 3:07-CV-3930 US Dist. Ct. NJ), portends the potential arrival of generic versions of Clarinex® in the highly-lucrative United States markets -- well-over $700 million in yearly Schering revenue -- much earlier than previously-forecast by Schering-Plough.]
Next, and more substantively -- Winston & Strawn (trial and patent counsel for many of the companies sued by Schering in this matter) has proposed an overall case management schedule, as set forth in the below letter -- in the event that US Magistrate Judge Tonianne J. Bongiovanni does not ultimately enter it, I will so report. For now, assume that this case schedule will hold.
WINSTON & STRAWN
August 26, 2008
BY ECF & FEDERAL EXPRESS
Honorable Tonianne J. Bongiovanni, U.S.M.J.
United States District Court
District of New Jersey
Clarkson S. Fisher Federal Building
& U.S. Courthouse
402 East State Street
Trenton, New Jersey 08608Re: Schering Corp. v. Sun Pharmaceutical Industries Ltd., et al.,
MDL No. 1851, Civil Action No. 07-cv-3930 (MLC) (TJB)
Dear Judge Bongiovanni:
We represent defendants Sun Pharmaceutical Industries Ltd. and Caraco Pharmaceutical Laboratories, Ltd. in the above referenced matter. We write Your Honor on behalf of the Plaintiff Schering Corp., as well as Defendants Mylan, Lupin, Perrigo, Orchid, Orgenus, Belcher, Geopharma, Sandoz, and Watson, seeking the Court’s approval of a summary judgment briefing schedule in this case. We do not write on behalf of Defendant Dr. Reddy’s Labs or Anchen.
Discovery has been proceeding since 2007, and the fact discovery period is set to expire on November 3, 2008. See Order Amending Scheduling Order (D.I. 293, 3:06-cv-04715-MLC-TJB). Expert discovery is then set to commence and expert reports are to be exchanged by mid-February. Id.
Defendants, with the exception of Dr. Reddy’s Labs and Anchen, and Plaintiff have agreed that, subject to Your Honor’s approval, the following summary judgment briefing schedule, as set forth in the enclosed Proposed Form of Order, would be appropriate: opening briefs to be filed no later than April 1, 2009, opposition briefs no later than May 1, 2009, and reply briefs no later than May 15, 2009.
If the enclosed Proposed Form of Order meets with Your Honor’s approval, we respectfully request that it be entered. Should Your Honor wish to discuss this matter, we would be happy to do so by phone or in person.
Respectfully submitted,
/s/ Melissa Steedle Bogad
Melissa Steedle Bogad
cc: All Counsel of Record (by email) (w/encls.)

UPDATED: I should have orginally noted that nothing in the above scheduling proposal letter makes an "at-risk" launch of a generic version of Clarinex RediTabs any less likely. The leading candidate -- of the existing defendants in this suit -- to possibly take that approach, is India's Orchid Pharmaceuticals.
Suffolk County, New York's RICO Suit Just Got a "Boost" From the Ninth Circuit. . . .
NOTE: This case, along with a host of others alleging consumer fraud, have now been settled by an agreed order, since approved by Judge Cavanaugh, requiring the payment by New Merck of money damages. This federal case file was thus closed, effective February 23, 2010.
However, the various putative class actions for securities fraud, and ERISA breach of duties cases, as well as the shareholders' derivative cases, and at least two Congressional investigations, and a host of civil governmental inquiries -- both state and federal -- remain open, active and ongoing.
You'll recall that, last month, this blog was the first (apparently worldwide!) to report on the filing of a lawsuit, by government officials in Suffolk County, New York [which county includes the glitzier environs of "the Hamptons" (uttered through clenched teeth, of course!)], against Schering and Merk, which in addition to Consumer Fraud and False Claims allegations, made RICO allegations -- calling these companies' conduct "indictable acts". [Click on thumbnail, below right.]
 While it has not yet happened, fairly shortly, Schering, et al., will make a motion in that suit -- a motion to dismiss for failure to state a claim under a federal Rule called 12(b)(6) -- saying essentially that counties generally have no standing to bring such a suit -- as the counties do not contract directly with the drugmakers for supplies of Vytorin or Zetia. The reasoning has heretofore generally run that only parties in contractual "privity" may generally sue on another, in such cases. Not so, held the Ninth Circuit Court of Appeals, just yesterday.
While it has not yet happened, fairly shortly, Schering, et al., will make a motion in that suit -- a motion to dismiss for failure to state a claim under a federal Rule called 12(b)(6) -- saying essentially that counties generally have no standing to bring such a suit -- as the counties do not contract directly with the drugmakers for supplies of Vytorin or Zetia. The reasoning has heretofore generally run that only parties in contractual "privity" may generally sue on another, in such cases. Not so, held the Ninth Circuit Court of Appeals, just yesterday.As Ed, over at Pharmalot notes this morning (albeit in another context), the County of Santa Clara, California has just won an important appeal against Astra USA, Inc., et al. -- Judge Raymond Fisher of the Ninth Circuit has held essentially that Santa Clara County was, in the words of Congress, a "directly intended third party beneficiary" of the main contract for the drugmakers' various drug products.
Thus, Santa Clara may sue the drugmakers directly -- and by inference, it just became far more probable that Suffolk County, New York will be able to survive the highly-predictable Schering motion to dismiss for failure to state a claim, under federal Rule 12(b)(6).
Cool. By the way, Schering-Plough, itself, was also one of the many other drugmakers sued in County of Santa Clara, California v. Astra USA, Inc. et al., ___ F.3d 11761 (Case No. 06-16471, August 27, 2008) -- here's a quote from the "business end" of the opinion:
. . . .Applying the federal common law of contracts, we hold that the covered entities are intended direct beneficiaries of these agreements and thus have the right to enforce the agreements’ discount provisions against the Manufacturers and sue them for reimbursement of excess payments. We have jurisdiction under 28 U.S.C. § 1291, and reverse the district court’s dismissal of the complaint under Federal Rule of Civil Procedure 12(b)(6) for failure to state a claim. . . .
. . . .As intended direct beneficiaries of the PPA, covered entities may enforce the Manufacturers’ ceiling price obligations under the federal common law of contracts. Although the statute mandating the PPA does not create a federal private cause of action, allowing Santa Clara’s contract claim to go forward is consistent with Congress’ intent in enacting the legislative scheme. Because it lies within the conventional competence of the courts, that claim is not within the primary jurisdiction of DHHS.
REVERSED and REMANDED.
Indeed -- Buckle-up, butter-cup.
Wednesday, August 27, 2008
Forbes' Herper (in Stereo!) on Vytorin Today. . . Cool.
Mr. Herper wrote earlier today on what September in Munich may mean to Vytorin (full SEAS trial data) -- tonight, he's writing about the lack of outcomes data for Vytorin. Does Matt know that something major is about to break on this ongoing debacle?
I dunno. Do read all of his latest -- here's a snippet:![]()
. . . .In SEAS, Vytorin failed to do better than placebo at treating a heart valve disease called aortic stenosis, but it did reduce the risk of heart attacks, strokes and operations to unclog arteries. But the results weren't much better than what you'd expect from Zocor alone. . . .
What does Matt suspect, that we've haven't yet puzzled out? Hmmmm. . . . Thoughts?
Forbes' Matt Herper -- On what Munich in September means for Vytorin -- SEAS
Do go read all that Herper has collected -- but there is nothing you haven't read earlier at Gooznews, here, over at Pharmalot, PharmaGossip, or over at Dr. Rost's joint (if you've been a steady visitor!) -- but good to see the MSM following the actual data, as opposed to the Schering/Peto "spin" on SEAS:![]()
. . . .Next week, the full results of SEAS will be presented at a medical meeting in Munich, and, if some of world's top cardiologists, drug safety experts and statisticians are to be believed, the stage is set for yet another battle over Vytorin, which is already being haunted by worries over its effectiveness.
Forbes surveyed 16 experts about the SEAS results. None were entirely convinced of a link to cancer, but eight thought Peto had gone too far in completely dismissing any cancer risk. Ten thought there was at least some possibility that Vytorin increases the risk of death for patients who have cancer. . . .
How could Zetia make cancers more deadly? One idea is that it is blocking substances that slow tumor growth. Zetia blocks the absorption not only of cholesterol, but also of substances called plant sterols, chemicals found in fruits and vegetables that may slow tumor growth. "It should push people further away from the use of the drug," says Allen J. Taylor, head of cardiology at Walter Reed Army Medical Center. But neither plant sterols nor a diet rich in fruits and vegetables have been proved to prevent cancer. . . .
Again -- Kudos go to PM -- for first articulating the theoretical mechanism of action mentioned in the last paragraph. . . You read it at Gooznews, first!
Once again, per PM: "Who Shells Out $15,000 For a Report Like THIS?"
First -- here's the report summary:
. . . .IntroductionThe antidyslipidemic market is expected to fall to $20 billion in 2017. The decline will be driven by the deep genericization of the market, further exacerbated by the patent expiries of the top antidyslipidemic, Pfizer's Lipitor, as well as by the recent negative messages from the ILLUMINATE and ENHANCE clinical trials. . . .
Highlights
Some 40% of the entire seven major market antidyslipidemic market is commanded by Lipitor, the gold standard therapy and highest selling agent among statins and antidyslipidemics in general. This will change dramatically after the loss of its patent protection in 2010/2011, reducing Lipitor's market share to 9% only by 2017.
The top 10 brands accounted for 81% of the market in 2007; the top revenue generating agents include Lipitor, Vytorin, Crestor, Zetia and Tricor. Over the forecast period the share of the brands in the antidyslipidemic market is expected to fall due to the further genericization.
The recent ENHANCE trial results have added to the distressing effects of genericization, while at the same time curbing the sales of Zetia and Vytorin, and further undermining confidence in the surrogate markers of atherosclerosis. This event is likely to make the ever-stricter process of approval for new agents even harder. . . .

Now, my answer to PM's poser:
Businesses that haven't yet figured out how to read Gooznews, Ed Silverman, over at Pharmalot, PharmaGossip and Dr. Peter Rost -- all for free.
That's who. Carry-on!
Tuesday, August 26, 2008
Via a Tip from PM -- "Silly Rabbit, Vytorin® is NOT for Kids!" Europe Nixes It -- for Children
 The FDANews is reporting that
The FDANews is reporting that
the European Medicine Agency’s
(EMEA) Paediatric Committee has
decided not to recommend use of
Vytorin®. . . for treating high cholesterol
in children. Quoth FDANews:The cholesterol drugs “do not
represent a significant therapeutic
benefit over existing treatments,” the
EMEA says in a statement. . . .
. . . .The drugmaker markets Vytorin
through a joint venture with Schering-Plough. . . .
Recently, two congressmen asked the
FDA to release a new study they say
links Vytorin to cancer. . . .
Ouch. Common sense makes a comeback, yes?
Organon's Raplon® Debacle: Of Lowenstein Sandler's Most Recent Inconsistent Arguments in an August 25, 2008 Memorandum of Law
 You'll recall that another well-regarded, largely successful litigation law firm was ultimately vexed by asserting, in an earlier reply memorandum of law, in this very case, that Schering may not have had the requisite level of notice/knowledge about the pre-acquisition Organon Raplon® woes, in order to render Schering a proper defendant in USA, et al. v. Organon, Inc., et al.
You'll recall that another well-regarded, largely successful litigation law firm was ultimately vexed by asserting, in an earlier reply memorandum of law, in this very case, that Schering may not have had the requisite level of notice/knowledge about the pre-acquisition Organon Raplon® woes, in order to render Schering a proper defendant in USA, et al. v. Organon, Inc., et al.
You'll also recall that that firm no longer represents Schering in the above Organon-Raplon matter. In papers filed with Judge Cavanaugh yesterday, Lowenstein Sandler, Schering's new counsel in the Raplon matter, once again argued that Dr. Feldstein has failed to allege that Schering had adequate notice of these pre-acquisition Raplon troubles (so as to ultimately be held liable for them).
Surprisingly, however, the first 15 or so pages of yesterday's filing essentially argue that three other civil suits (now settled) covered all this same ground -- and that those matters were so well-known to all the parties here, that Dr. Feldstein ought not be allowed to "stand on their shoulders", and allege the very same facts, in order to recover in his suit.
Well, that leads me to ponder -- "Which is it, folks"?
Did Schering not discover the Dr. Feldstein/Raplon/Organon troubles while conducting due diligence, during the Summer of 2007 -- before Schering paid almost $16 billion (as adjusted for less favorable currency exchange rates), in November 2007 for Organon's businesses -- or, were these earlier suits (and, by inference, Dr. Feldstein's putative claims) so well-known to the world -- Schering included -- that no suit should proceed? Take a look:
Me? I am shrugging, here.
I won't go on at any great length about it here, boring you with the "legalese" of how, in my opinion, Lowenstein is also conflicted about whether Dr. Feldstein should have to plead -- under federal Rule 9(b) -- with great particularity, about all these matters -- or whether it is enough, under the so-called "relaxed" 9(b) pleading standard, that Dr. Feldstein avers that essentially all of the most-important facts about what Organon knew (and did) relative to getting FDA approval for Raplon, despite some potentially very-lethal side effects. I'll simply note that Schering's position seems internally inconsistent on this front, as well.
Lowenstein Sandler argues, on the one hand, that Dr. Feldstein was an "insider" at Organon, and thus he should be required to provide, and prove, all the material factual details about what happened with Raplon, prior to and after, FDA approval (that would be the "with particularity" version of Rule 9(b)). On the other hand, Schering's firm, Lowenstein, argues that three other suits have resolved this matter -- at least one of those resulted in liability for Organon. So, again, which is it, folks? Is Dr. Feldstein allowed to assert at least some of what was found in the other suits to prove his, or must he provide all the evidence himself, without the benefit of any discovery from Organon's (now Schering's) files? 
Finally, Lowenstein argues that during the over four-year criminal investigation of these matters, by the U.S. Attorneys' Office out of Boston (and later, Manhattan), nothing apparently worthy of criminal indictments (or at least convincingly-provable) was uncovered. That should be rather "cold-comfort" for Judge Cavanaugh, given that this present version of the case is simply a civil matter -- thus, the heightened standards of proof, and specific-intent to defraud, applicable to criminal matters will not be applicable here -- in a civil matter.
Sunday, August 24, 2008


Saturday, August 23, 2008
So it's Biden -- That Ought to give Big Pharma pause. . . .
The online version of the Wall Street Journal is reporting that Sen. Joe Biden (D., DE) will be Sen. Obama's running mate. Buckle-up, as "fundamental, meaningful and deep" U.S. health care reform just became a far-more likely scenario in 2009 or 2010 -- from Sen. Biden's 2007 presidential campaign site:
. . . .Joe Biden’s highest priorities -– along with ending the war in Iraq – are universal health care and education. He will work bring together key health care stakeholders from labor, business, health care and government to seize the historic opportunity created by the recognition from organizations ranging from Fortune 500 companies, the Business Roundtable and the AMA to the labor movement that the time has come for universal, affordable health care. . . .
Negotiating For Prescription Drugs
The Medicare Part D prescription drug program was created in the Medicare Modernization Act of 2003. Medicare covers more than 40 million seniors and disabled Americans who are projected to consume $1.8 trillion worth of prescription drugs over the next decade. However, instead of using the purchasing power of 40 million Americans to get the best prices possible for prescription drugs, the Medicare and Modernization Act of 2003 expressly forbids the federal government from interfering in drug negotiations between pharmaceutical companies and the numerous private insurers spread out across the country that offer Part D coverage. Simply put, this “non-interference clause” dilutes Medicare’s bargaining position. The federal government successfully uses its bulk purchasing power to keep costs low in the Veterans Administration health system — why not allow it to do the same for our nation’s seniors who rely on Medicare?
In order lower prescription drug prices in the Medicare Part D program, Joe Biden will work to remove the prohibition against the federal government negotiating prices for prescription drugs for enrollees in Medicare Part D to allow the federal government to use its bulk purchasing power to reduce costs for Medicare beneficiaries. . . .
We can afford to provide universal health care in this country – and we can help pay for it with a national agenda of sensible steps to get skyrocketing health care costs under control.
The U.S. spends over $2 trillion on medical care every year – approximately $6,697 perperson. Health care is 16 percent of the gross domestic product (GDP). Health insurance expenses are the fastest growing cost component for employers. Premiums have gone up 78 percent since 2001 –- almost four times the rate of wages. In 2007, the average annual premium increased by 6.1 percent. Unless something changes dramatically, health insurance costs will overtake profits for many businesses by 2012. Yet we have no national agenda to address the affordable health care crisis. . . .
To reduce ever-increasing health care costs Joe Biden will create a panel to compare the effectiveness of medical treatments and technologies. This could be housed in an existing federal agency like AHRQ, NIH or HRSA, or it can be an independent, public-private partnership receiving funding from both the federal government and private industry. Many other countries — including Australia,Canada, England, and Germany — already require clinical and economic assessments of medical services as a condition for reimbursement. . . .

Indeed.
Now, just to be sure we're clear -- even in the increasingly-unlikely event that Sen. McCain were to win the White House, he too is keenly interested in significant cost-reforms -- disease treatment capitation, and increased price competition for drugs -- from his website:
. . . .Lowering Drug Prices. John McCain will look to bring greater competition to our drug markets through safe re-importation of drugs and faster introduction of generic drugs.
Providing Quality, Cheaper Care For Chronic Disease. Chronic conditions account for three-quarters of the nation's annual health care bill. By emphasizing prevention, early intervention, healthy habits, new treatment models, new public health infrastructure and the use of information technology, we can reduce health care costs. We should dedicate more federal research to caring and curing chronic disease.
Promoting Coordinated Care. Coordinated care - with providers collaborating to produce the best health care - offers better outcomes at lower cost. We should pay a single bill for high-quality disease care which will make every single provider accountable and responsive to the patients' needs. . . .
Yes, Mr. Hassan -- perhaps you should start preparing for federal government effectiveness panels setting mandatory best practice, lowest cost disease treatment protocols (for reimbursement), expanded drug price caps, remimportation from Canada, expanded generic-fostering legislation in the U.S., and possibly requiring clearly favorable "outcomes" data -- for new FDA drug approvals.
Friday, August 22, 2008
They Don't call "Motley" a "Fool" for Nothing. . . .

As Brian Orelli proved, once again
today, with his incoherent take
on the FDA and Congressional interest
in the Vytorin SEAS data on cancer.
Meanwhile, in the real world,
here's some more on the FDA
advance notification -- and more on
the Congressional request.
Yep -- "a fool is, as a fool does. . . ."
Thursday, August 21, 2008
Dr. Steve Nissen echoes PM's theory on Plant Sterols. . . .
 It seems this PM-generated theory just gained significant public intellectual currency. Excellent! Take a look at this CNN pull-quote, from Dr. Dr. Steve Nissen, chairman of the department of cardiovascular medicine at the Cleveland Clinic -- see the bottom of the article:
It seems this PM-generated theory just gained significant public intellectual currency. Excellent! Take a look at this CNN pull-quote, from Dr. Dr. Steve Nissen, chairman of the department of cardiovascular medicine at the Cleveland Clinic -- see the bottom of the article:
. . . .Nissen said one way Zetia may be linked to cancer is that it blocks the absorption of plant sterols. He explained, "There's a body medical literature that says those very plant sterols can inhibit the growth of cancer. . . ."
Let us now set about testing this possibility, without prejudice or rancor, and with the usual rigor we expect from truly independent scientists. Cool.
The Chairman Dingell/Rep. Stupak letters to Schering CEO Hassan and Merck CEO Clark, dated today. . . .
So -- circle September 4, 2008 in red on your calendar -- Schering will owe a repsonse by then. Note also that it seems another version of the "missing" study/trial patients issue has resurfaced.
Finally, it seems Schering-Plough's counsel's veracity, candor and commitment to completness, in oral representations -- is now being questioned, by two Congressional Committee Chairmen. Ouch.
Here it is, in full (H/T PM, at Gooznews):
Dingell, Stupak Question Drug Makers on Safety of Vytorin & Conflicting Study Data
NEWS RELEASE
Committee on Energy and Commerce
Rep. John D. Dingell, Chairman
For immediate release: August 21, 2008
Contact: Jodi Seth or Brin Frazier, 202-225-5735
Dingell, Stupak Question Drug Makers on Safety of Vytorin &
Conflicting Study Data
Recent Study Links Vytorin to Increased Cancer Risk
Washington, D.C. – Rep. John D. Dingell (D-MI), Chairman of the Committee on Energy and Commerce, and Rep. Bart Stupak (D-MI), Chairman of the Oversight and Investigations Subcommittee, today sent a letter to the CEOs of Schering-Plough Corporation and Merck & Co, Inc., requesting information about the safety and effectiveness of Vytorin, a prescription drug marketed by a joint venture of Merck and Schering-Plough.
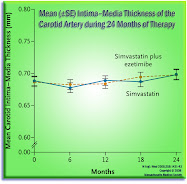
In a letter, Dingell and Stupak raise concerns about the results of the recent Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) study, which found Vytorin to be associated with significantly higher rates of cancer and cancer deaths than the placebo group. The lawmakers also requested clarification on conflicting and confusing study data.
"We are concerned that a study has found a significant link between Vytorin and cancer,” said Dingell. “Now it appears that Merck/Schering-Plough and its consultant are presenting two different data sets from this study to the public. Doctors and consumers should have better information on which to base their health care decisions."
"Vytorin's effectiveness has been in doubt, and now its safety is questionable,” said Stupak. “In addition, this may be another example of Merck and Schering-Plough playing with the release of a study's data. Patients and their doctors deserve full disclosure of the study data instead of competing press releases minimizing a potentially serious safety risk of Vytorin."

Now, the full text of today's letter is below.
~~~~~~~~~~~~~~~~~~~~~~
August 21, 2008
Mr. Fred Hassan
Chairman and CEO
Schering-Plough Corporation
2000 Galloping Hill Road
Kenilworth, NJ 07033
Mr. Richard T. Clark
Chairman, President, and CEO
Merck & Co., Inc.
One Merck Drive
P.O. Box 100
Whitehouse Station, NJ 08889
Dear Mr. Hassan and Mr. Clark:
Under rules X and XI of the Rules of the U.S. House of Representatives, the Committee on Energy and Commerce and its Subcommittee on Oversight and Investigations are continuing to investigate the safety and effectiveness of Vytorin, a prescription drug marketed by a joint venture of Merck and Schering-Plough (henceforth the joint venture).
We were concerned to learn from your own press conference that Vytorin wasassociated with significantly higher rates of cancer and cancer deaths than the placebo group in the Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) study, completed in June 2008. Although we appreciate the timely release of study results, we are troubled by the confusing nature of the information you released to the public.
For example, the SEAS press release from Monday, July 21, 2008, indicated that there were 93 cancer cases among those taking Vytorin and 65 among those taking placebo. The consultant’s press release from Oxford University’s Clinical Trials Service Unit (CTSU), however, indicated that there were 102 cancer cases among Vytorin users and 67 in the placebo group. Moreover, while the SEAS release provided a probability value (p-value) for statistical significance, the CTSU release did not.
Your counsel briefed Committee investigators about these results on July 22, 2008. During that briefing, your counsel asserted that the increased cancer deaths were an anomaly and that a report provided to the Food and Drug Administration (FDA) by Sir Richard Peto, co-director of the Oxford University Clinical Trials Service Unit, would support this position. Furthermore, your counsel advised that Dr. Peto’s report was not underwritten by the companies or the joint venture, and that it was submitted to FDA directly by Dr. Peto. Your counsel also informed the staff that the joint venture would not provide a copy to the Committee without assurances that it would not be released to the public. Furthermore, they encouraged the Committee to obtain a copy from FDA, which we have requested.
We are concerned that the analysis of Vytorin data conducted by Sir Richard Peto may not be as “independent” as expected, given that his Clinical Trials Service Unit is conducting the Study of Heart and Renal Protection (SHARP) trial of Vytorin, also funded by Merck, Schering-Plough, and/or the joint venture. In addition, Dr. Peto has apparently submitted a copy of his full report directly to FDA, but has not made it public, an action we deem questionable.
Therefore, we ask that you provide answers to the following questions:1. How much is Dr. Peto and his institute, the Clinical Trials Service Unit of Oxford University, being paid directly or indirectly by Merck, Schering-Plough, the joint venture, or their agents, attorneys, or lobbyists to conduct the SHARP trial?
2. Which data referenced above (SEAS or CTSU) are the correct data from which health care providers should base their clinical judgment?
3. What are the complete data for the number of randomized patients, as well as the number of cancers and cancer deaths, in each treatment arm of the SEAS, SHARP, and IMPROVE-IT trials?
4. Upon completion of the SHARP and IMPROVE-IT trials, will Merck, Schering-Plough, or its joint venture, conduct another full analysis of the relationship between Vytorin and cancer and cancer deaths based upon complete versus preliminary data?
Finally, please provide all records since January 1, 1998, relating to the following:1. All payments by Merck, Schering-Plough, the joint venture, or any of their agents, attorneys, or lobbyists to Dr. Peto or the Oxford University Clinical Trials Service Unit for any work related to Vytorin or for any other reason;
2. Any and all contracts or agreements between Merck, Schering-Plough, or the joint venture and Dr. Peto or the Oxford University Clinical Trials Service Unit for any work related to Vytorin or for any other reason;
3. All communications between Merck, Schering-Plough, the joint venture, or any of their agents, attorneys, or lobbyists and Dr. Peto or the Oxford University Clinical Trials Service Unit; and
4. All communications between Merck, Schering-Plough, the joint venture, or any of their agents, attorneys, or lobbyists and any Government officials related to the SHARP, IMPROVE-IT studies, or any work done by or on behalf of Dr. Peto or the Oxford University Clinical Trials Service Unit or any of their agents or contractors.
Please deliver copies of the requested records to the Subcommittee on Oversight and Investigations of the Committee on Energy and Commerce, Room 316, Ford House Office Building, no later than two weeks from the date of this letter. Please note that for the purpose of responding to this request, the terms “record” and “relating” should be interpreted in accordance with the attachment to this letter. After review of the records, we may require additional records and/or staff interviews with company officials.
Thank you for your prompt attention to this matter.Sincerely,


Ding! Ring the bell -- school's (almost) in session for Schering.
Excellent PharmaGossip Parody Image -- and FDA Advisory. . . .
I'll have excerpts from today's FDA's release here shortly, along with commentary and analysis. Until then, chuckle along with the Insider at PharmaGossip (and Fast Freddie!):
Jack prepared the above -- in response to mine, of this morning.
Quoth the FDA's current CDER page, on the topic, now:
August 21, 2008
Early Communication About
an Ongoing Safety Review
of Ezetimibe/Simvastatin
(marketed as Vytorin),
Simvastatin (marketed as
Zocor) and Ezetimibe
(marketed as Zetia)
FDA Investigates a Report from the SEAS Trial
This information reflects FDA’s current analysis of available data concerning these drugs. Posting this information does not mean that FDA has concluded there is a causal relationship between the drug product and the emerging safety issue. Nor does it mean that FDA is advising health care professionals to discontinue prescribing this product. FDA is considering but has not reached a conclusion about whether this information warrants any regulatory action. FDA intends to update this document when additional information or analyses become available.
FDA is investigating a report from the SEAS trial (Simvastatin and Ezetimibe in Aortic Stenosis) of a possible association between the use of Vytorin (a combination of simvastatin plus ezetimibe) and a potentially increased incidence of cancer. Simvastatin (Zocor), a “statin” class drug approved in 1991, decreases production of cholesterol by the liver and is indicated to reduce LDL-cholesterol levels and reduce the risk of cardiovascular events such as heart attack and stroke. Ezetimibe (Zetia), approved in 2002, inhibits the absorption of cholesterol in the intestine and is indicated to reduce LDL-cholesterol levels. Vytorin, the combination product approved in 2004, is indicated to reduce LDL-cholesterol levels.
Recently, FDA obtained preliminary results from the SEAS trial. This clinical trial tested whether lowering LDL-cholesterol with Vytorin would reduce the risk of major cardiovascular events, including aortic valve replacement, congestive heart failure, and ischemic cardiovascular events in individuals with aortic stenosis (a tight heart valve). A lower overall cardiovascular risk was not found with Vytorin. However, there was an additional observation that a larger percentage of subjects treated with Vytorin were diagnosed with and died from all types of cancer combined (including skin cancer) when compared to placebo during the 5-year study.
Interim data from two large ongoing cardiovascular trials of Vytorin – the Study of Heart and Renal Protection (SHARP) and the Improved Reduction in High-Risk Subjects Presenting with Acute Coronary Syndrome (IMPROVE-IT) – show no increased risk of cancer with the combination of simvastatin plus ezetimibe. The SHARP trial is expected to be completed in 2010. The IMPROVE-IT trial is scheduled for completion around 2012. Safety data from both of these trials are being evaluated on a regular basis by independent data safety monitoring boards. FDA has determined that, to date, these findings in the SEAS trial plus the interim data from ongoing trials should not prompt patients to stop taking Vytorin or any other cholesterol lowering drug.
FDA is aware of previous reports suggesting a link between low on-treatment cholesterol levels and an increased risk of cancer. A 2007 pooled analysis of 16 studies with 23 statin drug arms, published in the Journal of the American College of Cardiology, reported an association between the level of LDL-cholesterol achieved and incident cancer in patients receiving a statin.
However, most large prospective studies of statin drugs have reported no difference in cancer incidence between the active and placebo arms. For simvastatin, the Heart Protection Study randomized 20,000 patients to a daily dose of simvastatin 40 mg or placebo for up to 5 years. The incidence rate for cancer was 7.9% in the simvastatin group and 7.8% in the placebo group, and the deaths from cancer occurred at similar rates in both groups.
FDA anticipates receiving a final SEAS study report from the sponsors in about 3 months. Once FDA receives the final study report, it will likely take 6 months to fully evaluate the clinical trial data and other relevant information. As soon as this review is complete, FDA will communicate our conclusions and recommendations to the public.
An elevated LDL-cholesterol level is an established risk factor for heart disease and lowering cholesterol reduces the risk of death from heart disease and stroke. Patients should not stop taking Vytorin or other cholesterol lowering medications and should talk to their doctor if they have questions about whether to continue to take the medication. Until further information is available, healthcare professionals and caregivers should continue to monitor patients taking Vytorin as outlined in the prescribing information.
The FDA urges both healthcare professionals and patients to report side effects from the use of Vytorin to the FDA's MedWatch Adverse Event Reporting program
The FDA urges both healthcare professionals and patients to report side effects from the use of Vytorin to the FDA's MedWatch Adverse Event Reporting program
- on-line at www.fda.gov/medwatch/report.htm
- by returning the postage-paid FDA form 3500, available in PDF format at www.fda.gov/medwatch/getforms.htm to 5600 Fishers Lane, Rockville, MD 20852-9787
- faxing the form to 1-800-FDA-0178
- by phone at 1-800-332-1088
References
~~~~~~~~~~~~~~~~
Alsheikh-Ali A., et al. -- Effect of the magnitude of lipid lowering on risk of elevated liver enzymes, rhabdomyolysis, and cancer. J Am Coll Cardiol 2007;50: 409-18.
Heart Protection Study Collaborative Group -- MRC/BFH Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomized placebo-controlled trial. Lancet 2002;360: 7-22. . . .
Indeed. So, sit tight for about nine more months, at least. As ever, more to come.
Pharmalot: New Insights on Low LDL and Cancer Incidence
 You'll recall that Vytorin's SEAS trial raised the spectre of elevated cancer incidence rates being associated with Vytorin's cholesterol lowering "therapy". You'll also recall that Schering's experts were, in the view of many independent observers (Dr. Roy Poses among them) astonishingly cavalier in their high-handed, and essentially instantly-appearing dismissals of any cause-effect link between the two.
You'll recall that Vytorin's SEAS trial raised the spectre of elevated cancer incidence rates being associated with Vytorin's cholesterol lowering "therapy". You'll also recall that Schering's experts were, in the view of many independent observers (Dr. Roy Poses among them) astonishingly cavalier in their high-handed, and essentially instantly-appearing dismissals of any cause-effect link between the two.
If you are a regular reader, you may also recall that PM, over at Gooznews, recently posited an fascinating "mechanism of action" theory to explain these elevated cancer incidence observances -- a mechanism that involves plant sterols. This morning, Ed Silverman at Pharmalot fills-in a new, and important piece of this complex puzzle. Do go read it all, but I found this snippet to be pretty interesting, if oblique, support for PM's emerging plant sterols theory:
. . . .“While statin treatment in itself appears not to increase the risk of cancer, the issue of a possible link between very low LDL-C levels and cancer has not been fully resolved,” they wrote. “Given the importance of the topic, it is paramount that the Food and Drug Administration and the pharmaceutical industry promptly analyze and report the cancer incidence in the various trials”. . . .
[Emphasis supplied.]
Now recall that Vytorin's mantra has long been that "lower is always better", when it comes to LDL levels.
It may be time to debunk [KUDOS go to the Insider, at PharmaGossip!] that sound-bite. Actually, Drs. Anthony DeMaria, editor-in-chief of the Journal of the American College of Cardiology, and Ori Ben-Yehuda, of the University of California, San Diego Medical Center, seem to have just done so.
Wednesday, August 20, 2008
CNBC Runs a Favorable Investment Opinion Piece on Schering-Plough -- Quoting A Fifth-Third Fund "Portfolio Manager" -- but fails to disclose. . . .
I am not certain that these two are affiliates, but it certainly seems likely. . . .
Earlier today, a Fifth Third Disciplined Investment Fund "Portfolio Manager" named Scott Richter said he "likes" Schering-Plough's management, in this CNBC piece. Okay. Take a deep breath, now. That's right -- he is basing his favorable commentary on the strength of Schering-Plough's "management". R-i-i-i-i-i-ght.
Obviously, that struck me as a very unusual thing to say, given what we all now know. So I set out to do some digging.
When CNBC first ran this pro-Schering piece, it indicated that "disclosure information was not available for Richter, or for his company. . . ." [Emphasis supplied.]
Not so. See the SEC website. Richter was the person quoted, on behalf of the entity -- the Fifth Third Fund (presumably, some investment vehicle-affiliiate of the Fifth-Third banking entities). As a threshold matter -- why would CNBC run the piece, then? Forget the SEC rules requiring such disclosures (of "portfolio managers" making public comments), for a minute -- isn't that a Journalism 101 question: "What is your stake, if any, in the company you are touting?"
In any event, we find this, over at the SEC -- look at the following alphabetical listing -- of holdings by Fith Third Asset Management, presumably an affiliate of that firm's Disciplined Investment Fund:
SCHERING-PLOUGH
Quarter Ended June 30, 2008
$29,315,000 Value
1,488,826 Shares
Sole Investing Decision Authority;
Sole Voting Authority on all.
~~~~~~~~~~~~~~~~~~~~
Quarter Ended March 31, 2008
$1,190,000 Value
82,551 Shares
Sole Investing Decision Authority;
Sole Voting Authority on all.
Fascinating. Fifth Third entities acquired just over 1.1 million shares between March 31 and June 30, 2008 -- in the most-recent quarter. Moreover, the March 31, 2008 shares carry an average value of $14.41 per share -- and the June 30, 2008 shares show an average per share value of $19.69. Do you think Fifth Third is motivated to see Schering stay above $20 per share? I do. And that, my friends, is material information.
[DELETION -- 09.16.08]
It would seem that Fifth-Third might have over $29 million reasons to want to see this stock rise. . . . but citing "management strength" might be the least convincing one of all.
[CORRECTED: 09.16.08 9 AM:
Now — John Puskar, in a comment to the back up site, on wordpress — informs me that I was wrong about which Scott Richter this involves. My most sincere apologies. The story is accurate; I have the wrong Scott. A different Scott Richter was the Fifth Third analyst, so I've removed the matter that used to appear below, and put it in a comment -- the text is there to preserve the record, just to be clear. Again, my apologies. -- Condor]
More on Salmon's keen observations -- of strikingly-similar chemical compound structures -- from last week. . . .
I admit that I have been rather dilatory in rendering some graphics, here, in order to help amplify a very-cogent (if deeply chemical) point offered by Salmon, last week, in our comment-box, for all of us "NON-rocket scientists" to see, more clearly. I am a visual learner -- I am sure others are, as well.
So, finally did I stay up late last night, to complete the glossy, three dimensional rendering of Vertex's teleprevir, and then twisted the rendering in space, on the page, to highlight just how strikingly-similar (though slightly shorter, and thus less-cluttered, or simpler) the competing Schering-Plough candidate, boceprivir, is to the Vertex candidate. Vertex's is labeled VX-950 -- teleprevir. Look first at it -- click to enlarge:
Okay -- now recall the rendering I created last week, for the "Name that Compound" trivial pursuit contest -- it is the Schering candidate, called "boceprivir":
Do you see -- especially nearest the mid-points of the two compounds -- the striking "familial resemblance"? So do I.
Now, read what Salmon wrote:
. . . .I'm so glad you're talking about mechanisms.
. . . .I do want to discuss a little bit about boceprivir.
This weekend I was thinking that for several different companies to all come up with structurally similar drugs for Hep C around the same time means that they all have a common mechanism that they're basing it on and the it must involve the part of the structure that's similar across molecules.
Then it struck me. Zyprexa, Lilly's wonder drug and that favorite of prosecutors and personal injury lawyers everywhere was noted to not only cause weight gain and diabetes in the original summary basis of approval. But it also caused severe liver toxicity in several people who were Hep C positive and structurally it has a metabolite that's very similar to boceprevir and the other ...previrs. Not only that, but there's a lot of information in the scientific literature that points to the same thing. In fact after Zyprexa, drug companies and FDA only started using people with non Hepatitis induced liver disease (e.g. alcoholic cirrhosis only) in hepatic impairment studies with new drugs and also began screening Hep C patients out of clinical trials.
I would absolutely bet my house that someone in FDA knows something about this and has been helping drug companies cover this up for the last 12 years or so.
The information is right there on the FDA's website. All anyone needs to do is look at the original reviews for Zyprexa and look at the metabolism of the quaternary Nitrogen. (In case anyone's interested just google Drugs@FDA.). . . .
-- Salmon
Salmon went on to write that he worried that much of this FDA reference material just might vanish into the ether -- if it were widely-seen, and well-understood. Let us now conduct that experiment. Will the FDA remove any, or all, of that linked material? I, for one, am skeptical. But, as ever, we shall see.
~~~~~~~~~~~~~~~~~
A Houseekeeping Note: I have placed a black-backgounded-version of the graphics here for PharmaGossip, and Peter Rost. Hint, hint. . . .]
Tuesday, August 19, 2008
Teleprevir starts second Phase III trial -- extending lead over Schering's Boceprevir. . . .
 This morning, Johnson & Johnson, in partnership with Vertex, announced that FDA consented to Vertex's trial design for medicating a second set of patients (these being that are not Hep-C treatment naive) in its ongoing Phase III trials. . . . Quoth Reuters:
This morning, Johnson & Johnson, in partnership with Vertex, announced that FDA consented to Vertex's trial design for medicating a second set of patients (these being that are not Hep-C treatment naive) in its ongoing Phase III trials. . . . Quoth Reuters:
. . . .Vertex reiterated that it is on track with its previously stated plan of filing for approval of the drug in the second half of 2010 based on data from a Phase III, or late-stage, clinical trial of the drug in patients who have not previously been treated.
Zachry Barber, a spokesman for Vertex, said the company has not provided a timeline for completing its latest trial, called Realize, but said it expects to complete enrollment of 650 patients with the most common form of the liver-destroying disease in the first quarter of next year.The trial will be conducted in the United States and Europe and compare two 48-week telaprevir-based regimens with a 48-week control arm. . . .

This puts Schering's boceprivir even further behind the 8-ball. . . . More background on this horse-race here.
Monday, August 18, 2008
July 2008 IMS Data -- Vytorin®/Zetia® market share continues to melt -- month over month. . . .

Schering just released its July 2008 US cholesterol management market IMS data. The data includes only about five selling days after the SEAS Trial disappointment/announcement, so this month's data cannot be relied upon as representative of how August will turn out.
That said, the overall US cholesterol management market grew slightly, July over June -- and again, Vytorin®/Zetia® actually lost share, July over June -- despite being up a fraction of a percent in raw scrips. [This "losing share" trend was also seen in the June 2008, over May 2008, IMS data.]
More precisely, Vytorin/Zetia represented about 11.72 percent of the US cholesterol management presecription market in July, down from about 12.1 percent in June 2008.
That is bad news. Graphics -- with more trendline detail -- coming shortly, right here. Stay tuned. See above. And below.
UPDATED -- 08.19.08 @ 8 AM EDT
~~~~~~~~~~~~~
Overnight, The Insider, at PharmaGossip linked this post, and featured an earlier draft version of the above graphic! Cool!
Next, Ed over at Pharmalot, has a nice analysis of the melting Schering market share issue, this Tuesday morning -- and so, I thought I'd amplify one point of his, from yesterday -- and sythesize it with this -- all of it probably being lost on the casual reader of that fine site:
Yesterday, Pharmalot noted that a consulting firm has labeled Schering's pipeline the "deepest" in the business -- it has the most potential to be self-replenishing by 2012. For the moment, let's assume that is true.
To bring the number -- and variety -- of drug candidates to approval by 2012 -- that these consultants (and Schering, itself) forecast, Schering will need massive cash-flow generation mechanisms -- perhaps $2 to $3 billion per year, every year -- over and above the cash-flow needed for ordinary operations.
That "machine" was to be Vytorin. No more. As US market share melts, like an ice cream sandwich, in the August heat on the beaches of Fire Island. . .
I wonder, honestly, which of those "fan-tabu-licious" new drug candidates are going to have to be shelved -- or scrapped -- for lack of cash flow to bring them forward, fast enough -- all by 2012.
Schering's own recent SEC filings (see page 27 of the most recent Form 10-Q, at the end of the fourth full paragraph) plainly warn that Schering is "substantially dependent" upon Vyotrin -- to fund its future pipeline delivery strategy.
That may be the meta-narrative, here.
Saturday, August 16, 2008
Insider at PharmaGossip has "the BIZ-ness"! Faux DTC spot for Vytorinoxil®*!
Excellent fun -- courtesy a link provided by the Insider, at PharmaGossip!
We bring you -- with no further ado -- Vytorinoxil®*!
~~~~~~~~~~~~~~
* Any resemblance in this Holton Sentivan + Gury spot -- to any actually-marketed brand name pharmaceutical. . . . is entirely coincidental. I swear. Cheers!
No Doubt About It -- London 2012 will have quite a time topping that!
We break format, to wander "Off-Topic" (as we are wont to do, about once every three months or so) here -- and simply note: if you weren't amazed, tonight -- you mustn't have an EKG pulse:

Forget the politics for a moment -- that was quite the post-card for the world's most-populous unified economy.
And, if you've ever competed, at any level, you couldn't help but feel the butterflies -- as each of the nation's athletes entered the Bird's Nest. . . . And. . . we're underway. Wow.

UPDATED:

Now, an update on the "Wow" factor: If Jamaican Usain Bolt (click on image, above) can smoke the world mark while coasting, thumping his chest, and spreading his arms -- while the "race" is still underway -- in the final nine meters, before crossing the tape -- how far deep into nine-four land can he go, if/when he is still accelerating during those final three strides? Prepare to see the 100 meter (and 100 yard) record books completely re-written -- and they'll all read "Bolt 2008". Amazing. Imagine this guy in a 40 -- at an NFL combine -- He'll run near a 3.8 40. Whoah. I wonder how fast he'd be in pads. . . . Bolt can write his own ticket, now.
Thursday, August 14, 2008
Although A Jim Cramer "Recommendation" is USUALLY an Excellent CONTRA-Indicator -- Do Consider Vertex's Case as a "Long". . . .
I reflexively cringed -- while typing his name into the header for this post -- as he was so completely wrong, and repeatedly-brazenly wrong, about Schering itself. . . . but the below suggests he may have learned at least one thing from that debacle of his (and Schering's) -- continued flogging of a failing stock story. Take a look. I'll admit that this is exactly how I see Vertex. And, I'll admit that I am neither long or short Vertex, Abbott, Astra Zeneca or Schering, at the moment.
. . .Cramer defended the stock today, claiming Wall Street misread some recent study data and took Vertex down unnecessarily.
. . . .The test designs were different, and Schering had fewer test subjects and lower drop rates. Also, Vertex’s drug seemed to have less severe side effects. And Teleprevir works on patients with treatment-resistant hepatitis C, while Schering’s drug does not. That means Vertex had virtually exclusive access to the 300,000 Americans who fit that description. And, on top of all this, Teleprevir is much closer to market than Schering’s drug. In the U.S. alone, the expected sales top out at $1.2 billion. . . .
There. For. What. It. Is. Worth.
Abbott to Co-Promote Crestor® in the US. . . .
And that will spell [more] bad news for the Vytorin/Zetia franchises. Astra Zeneca's Crestor® will now be part of Abbott's marketing juggernaut in the United States -- via Reuters' reporting, this morning:
. . . .Abbott will obtain the nonexclusive right to promote Crestor® alongside AstraZeneca in the United States, excluding Puerto Rico. Terms were not released.
Sales of Crestor®, Astra's third-largest drug, soared 35 percent to $916 million in the second quarter.
Crestor sales have been benefiting from surprisingly [but not to regular readers of this blog -- see this much earlier item! -- Ed.] positive clinical trial results and from setbacks involving Vytorin, a rival cholesterol drug sold in partnership by Merck & Co and Schering-Plough Corp.AstraZeneca said the deal would enable it to leverage Abbott's presence among doctors who prescribe cholesterol medicines.
Abbott, based in suburban Chicago, also sells Niaspan®, for raising "good" cholesterol, and TriCor®, which targets triglycerides.
The companies in 2006 announced an agreement to develop a combination pill melding the main ingredients in Crestor® and TriLipix®, a next-generation version of TriCor®. They plan to seek U.S. approval for the product in the second half of next year.
An application for Abbott's TriLipix® is under U.S. regulatory review as a single product. . . .
[Emphasis supplied.]

I suspect Schering's July IMS 'scrip data (due out very shortly) will show renewed, and additional, erosion in the Vytorin/Zetia franchises, after the disappointing July 21, 2008 SEAS trial results.
[For an earlier item on Abbott's invasion of another Schering franchise, see this post -- and the small graphic, at left. It seems Abbott's Humira®, is effective for at least a three year duration, in treating ankylosing spondylitis (AS) -- an indication, disease and/or condition for which Schering has a drug candidate (not yet approved) in Europe. As Schering seeks EU approval, it is certain that the EU authorities will take note of the efficacy of the tried and true Humira® -- already there approved, and consider whether Schering adds anything of significance to the mix. In Europe, because country-level governments are the most important payers, cost/benefit is far more likely to be a factor in EU regulatory approvals.]
Monday, August 11, 2008
PM, at Gooznews, has an intriguing theory. . . .
The irrepressible PM (over at Gooznews.com) strikes again, this morning -- the author has posited an intriguing "mechanism of action" theory to explain why the SEAS cancer data may not be an anomaly at all, among other matters. It involves plant sterols. Trust me, you'll want to read this -- this one post may well cause "serious, open minded scientists" to rethink what Schering-Plough is claiming, related to the SEAS cancer data. Here's a bit of it:
. . . .The trial -- known as the SEAS trial -- was an effort to show the combination pill reduced heart disease. Ezetimibe is unique in that it inhibits cholesterol absorption (as opposed to removing cholesterol from the blood like statins). But ezetimibe also inhibits absorption of dietary plant sterols, and one plausible theory is that the reduction in sterol absorption in the patients in the SEAS trial may have increased their risk of contracting cancer. . . .
Excellent.
Sunday, August 10, 2008
Sandoz seeks Declaratory Judgment that Schering-Plough's Clarinex® Patents are Invalid. . . .
 This past week, Sandoz answered Schering-Plough's patent lawsuit titled In Re Descloratadine Patent Litigation (MDL No. 1851 Civil Action No. 07-3930), by asserting, among other matters, that both of the principal patents Schering relies upon in manufacturing and marketing the Clarinex® products (the so-called '463 patent, and the '274 patent) are invalid -- and thus unenforceable, at least as to Sandoz -- chiefly for procedural defects in the way Schering handled its FDA Orange Book notices, and then subsequently failed to include some of the materials listed in the Orange Book submissions -- in its infringement complaint against Sandoz.
This past week, Sandoz answered Schering-Plough's patent lawsuit titled In Re Descloratadine Patent Litigation (MDL No. 1851 Civil Action No. 07-3930), by asserting, among other matters, that both of the principal patents Schering relies upon in manufacturing and marketing the Clarinex® products (the so-called '463 patent, and the '274 patent) are invalid -- and thus unenforceable, at least as to Sandoz -- chiefly for procedural defects in the way Schering handled its FDA Orange Book notices, and then subsequently failed to include some of the materials listed in the Orange Book submissions -- in its infringement complaint against Sandoz.
The Sandoz answer also asserts that the so-called '274 patent held by Schering is generally invalid, and thus presents no barrier to Sandoz's planned generic Descloratadine [or, Clarinex®-equivalent] product.
Interesting. As ever, more to come.
Subscribe to:
Posts (Atom)